
A very common condition that occurs in approximately 3% of the population. Despite this the cause of the condition remains unknown. It most commonly occurs in people over the age of 40 years and is more common in women and more common in diabetics. The good thing is that the condition usually occurs in an otherwise normal shoulder, so X-rays and ultrasound scans are often normal.
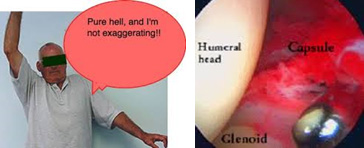
The most common symptom is painful stiffness of the shoulder. The pain is often worse at night, worse at the extremes of movement, and worse with sudden movements. Generally, a global loss of range of motion of the shoulder occurs, but the extent of motion loss is extremely variable, and depends to some degree on the extent of inflammation in the lining of the joint (the capsule).
As a general rule the condition is self-limiting, which means that it will eventually get better even without any treatment. However, the natural history can be very prolonged, and in the worst cases it may last for 3 to 4 years. The condition can occur in both shoulders in up to 15% of people, but usually not at the same time.
Typically, the pain begins first and slowly gets worse; loss of shoulder movement then follows. In the early stages before loss of motion occurs the condition is commonly confused with shoulder bursitis and impingement. The only other condition that causes a true painful stiffness of the shoulder is shoulder arthritis.
The most important aspect of treatment is patient education to ensure the patient understands that the condition will get better by itself. It is important to continue to use the arm within the limits of comfort and not stop using it. Regular analgesia and the use of anti-inflammatory tablets can help with the pain, and gentle stretching exercises will help to recover movement.

Physiotherapy often makes the pain worse, and in general there is no point trying to aggressively stretch tissues that are in essence very inflamed. Probably the most useful treatment is to get an intra-articular (into the joint) injection of cortisone. Injections into the subacromial space as is commonly done for bursitis and impingement will not help – the injection must be into the joint. This is very effective at stopping the inflammatory component of the condition which will make a big difference to the pain. Movement recovery will then follow but will still take some time.

The only quick way to get movement back is with surgery. During the operation, an arthroscopic (keyhole) release is performed to cut all the thickened capsular tissue that lines the joint. This is the tissue that restricts shoulder motion. However, given that in the vast majority of people the condition will get better by itself surgery is rarely required.