
The shoulder joint is a complex structure that allows for a wide range of arm motion and strength. It is the most mobile and flexible joint in the body. To allow this mobility the shoulder has a large humeral head (ball) which forms a joint with a small flat glenoid (socket), a bit like a golf ball on a tee. As a result the shoulder is vulnerable to injury, particularly instability.
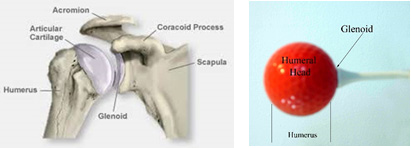
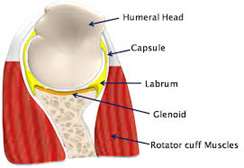
The head of the humerus is normally held firmly in place in the glenoid by ligaments that connect the humerus to the shoulder blade, rotator cuff tendons that connect the muscles of the shoulder blade to the humerus, and a rim of cartilage (labrum) that encircles the glenoid, increasing the depth of the socket.
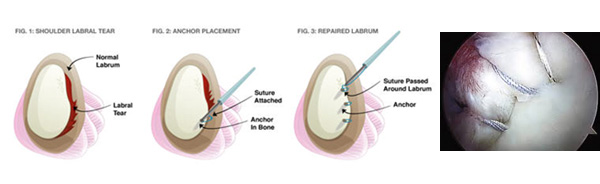
Shoulder instability is a very common problem in the young athletic population. This results when the shoulder has come out of joint (dislocation) or tried to come out of joint (subluxation), usually following a traumatic injury. As a result there is often damage that occurs to the supporting structures of the shoulder, most commonly the labrum and attached ligaments. This can then result in recurrent episodes of instability, which not only cause pain and disability, but can result in progressive damage to the shoulder joint.

For symptomatic shoulder instability there are 2 options for treatment:
Non-Operative Treatment
Because the torn labrum and ligaments do not heal by themselves non-operative treatment is generally not successful in preventing recurrences, especially in the young athletic population. It aims to restore range of motion in the shoulder and strengthen the rotator cuff and scapula muscles (dynamic stabilisers) so that they can better assist with stability and control. Although this form of treatment may be effective in patients with low physical demands, it rarely results in long term stability for younger more active patients who require the support provided by the damaged structures (static stabilisers).
Operative Treatment
The primary aim of surgery is to restore shoulder stability and function by repairing the damaged structures back to where they should be. This is done by using little absorbable ‘suture anchors’ which are inserted into the glenoid. The sutures from these anchors are then used to attach the ligaments and labrum back to the bone. The procedure normally takes from 60 to 90 minutes, and is most commonly done through key holes (arthroscopic). If there has been damage to the bone of the glenoid from multiple instability events then occasionally a bone graft has to be performed to restore bone support. This is done through a small cut over the front of the shoulder.
Recovery after Surgery
Shoulder stabilization surgery is normally a very safe and successful operation, and is one of the most common operations that I do, but it does involve a long recovery and rehabilitation period. Usually you will need to be in hospital for only one night after the operation. I will provide you with information sheets and exercise sheets before you leave the hospital which will outline very clearly how to look after your arm following the surgery.
As a brief outline:
You will spend the first 4 to 6 weeks with your arm in a sling. This will only be removed for showering purposes or when you are doing your exercises. You cannot drive during this period.

You will then spend another 4 to 6 weeks limited to very light waist level use of the arm. This is to allow further healing of the tissues whilst you continue to work on regaining ‘passive’ range of motion in the shoulder. You will be able to start driving and do very light desk type of work during this period.
More formal rehabilitation including stretching in other planes and strengthening does not begin until the 10 to 12 week mark. This is when physiotherapy can also be helpful. It can take 4 to 6 months before you are back doing more physical activities with comfort and a good mobility, and you are not allowed to return to sport for 6 months. This is because the tissues that have been repaired are not fully healed until 6 months.
AC Joint Stabilisation

Acromioclavicular (AC) joint stabilisation is a surgical procedure employed to treat severe cases of AC joint dislocation. AC joint dislocation is the separation of the collar bone or clavicle from the acromion (the top portion of the shoulder blade or scapula at the outer edge of the shoulder) due to severe trauma. AC joint dislocation usually occurs as a result of a direct fall on to the top of the shoulder which causes the shoulder blade to be forced downwards and the collarbone to pop up.
You will need the Adobe Reader to view and print these documents. 